Thursday, September 10, 2009
What is "Endocarditis"?
I have an artificial valve -- do I need to take blood thinners?
What is the best kind of artificial valve?
The need and ability to maintain long-term anticoagulation (blood thinning) is a very important factor. Several classes of people may not be good candidates to take warfarin (brand name coumadin), and therefore should receive a bioprosthetic valve. This group includes young women who wish to become pregnant. They should not take warfarin since it can frequently cause birth defects. Some people wish to continue to lead very, very active lives and taking a blood thinner would complicate the ability to do so. People who have had previous and sometimes repeated problems with bleeding (for example, frequent bleeding from ulcers) are often felt to be better served with the bioprosthetic valves which do not require anticoagulation.
On the other hand, for people who are going to need to have anticoagulation anyhow because they have the abnormal rhythm known as atrial fibrillation, using a bioprosthetic valve would have little advantage since they are going to need to take the blood thinner anyhow. They will most often receive a mechanical valve to take advantage of its longer life.
Another consideration for some people is the efficiency of the valve. That is, the replacement valve is never as good as the "real thing" in terms of how well it opens. Some artificial valves obstruct the flow of blood quite a bit, while others (mainly some of the bioprosthetic varieties) obstruct very little. There are some world-class athletes who compete despite having artificial valves, and they will have one of these "low profile" valves utilized to avoid loss of efficiency. This is generally not a consideration for most of us.
What kinds of artificial valves are there?
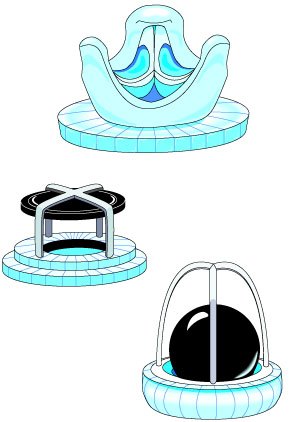
Mechanical valves. There are several different varieties, including "bileaflet tilting valves" which are extremely popular and reliable. Tilting single disc devices are also quite popular. Older models included the "caged-ball" device and "floating discs". The body does not recognize these as "foreign", and thus there is not a fear of rejection. Mechanical valves are generally felt to have the advantage of lasting the longest time. Their main disadvantage compared to other types of valves is the need to take potent blood thinners which decreases the tendency to form clots on their surface.
Bioprosthetic valves. These use some biologic material in their composition. They are all treated, and do not carry the risk of rejection. Treated aortic valves from human cadavers, treated pig aortic valves, and valves fashioned from the pericardium (the outside lining of the heart) of cows are all utilized. These types of valves do not necessarily require that the patient take blood-thinners, but generally do not last as long.
Please note that there are pictures of various valves below.
What kinds of surgery are available for problems with the Aortic Valve?
The Ross procedure. The Ross procedure utilizes the patient's own pulmonic valve for replacement into the aortic position.
Balloon aortic valvuloplasty. Balloon valvuloplasty of the aortic valve is an attractive technique for aortic stenosis since a large number of people with this problem are quite elderly and thus not ideal candidates for surgery. However, these same patients also typically have a heavily calcified aortic valve, and strokes secondary to loosening of this material can occur. Unfortunately, there is also a higher recurrence rate, with up to 80% of patients requiring repeat procedures within 6 months.
What kinds of surgery are available for problems with the Mitral Valve?
Mitral valve repair. In many cases of mitral regurgitation, the problems that cause leakage can be repaired by a skilled surgeon without the need for replacement. Often, a valve "ring" is placed in the orifice that the mitral valve covers to "tighten up" the size of this area and allow the valve to cover it more effectively. The size and shape of the leaflets can be carefully remodeled, and torn structures sewn back together. Repair offers the advantage of improved left ventricular muscle performance, since the muscle (papillary muscles) and supporting structures (chordae tendiniae) are left intact. The long term results of repairing and saving the person's original "native" valve is often better than repair, with improved heart muscle function and decreased need for repeated surgical procedures. Furthermore, after repair there may be no need for long term anticoagulation. It is important to discuss this with your surgeon if you are planning to have surgery for mitral regurgitation.
Mitral commissurotomy. During this procedure, which is done for some people with mitral stenosis, the leaflets which have fused together at their "commissures" (points of touching) are separated by the surgeon. Like mitral valve repair for regurgitation, not all cases are suitable candidates for this approach, as sometimes the mitral valve is too calcified, or the leaflets cannot be separated in a satisfactory manner. Nowadays, many candidates for commissurotomy are treated with balloon mitral valvuloplasty.
Mitral valve replacement. Some mitral valves simply need to be replaced. This may not be known until the actual time of surgery, when a repair for regurgitation or a commisurotomy for stenosis can then be seen to be impossible or ill-advised. The valvular structure is cut out, and as much of the supporting structure left as feasible. The new valve may be mechanical or bioprosthetic (see explanation and picture below), and may be done from a standard approach across the breastbone ("median sternotomy"), or with some of the new "mini" approaches.
Balloon mitral valvuloplasty. This procedure is done in a manner similar to balloon coronary artery angioplasty. That is, access is gained to the circulation from the vessels in the legs, and a catheters with deflated balloons are advanced through the vessels to a position across the mitral valve. The balloons are then inflated, creating a somewhat uncontrolled but effective commissurotomy as described above. This all obviously occurs without having to enter the chest surgically, and is much easier on the patient in most cases. Again, not all people are candidates for balloon angioplasty, particularly those with heavily calcified valves. However, it is gaining increasing popularity in many centers.
Myocardial reduction procedure with mitral valve replacement (Battista procedure). In some cases of cardiomyopathy and congestive heart failure, the heart's natural tendency to dilate becomes massive, and becomes a problem of itself. It is often associated with substantial leakage through the mitral valve, as its annulus dilates. Battista, a surgeon in South America, pioneered a surgery which actually cuts out a very substantial part of the heart muscle, restoring it to a more efficient size. The mitral valve is also often removed in the course of this surgery. Although it is counterintuitive to cut out muscle from a weak organ, initial experience has been favorable.
What kinds of medications are available for valve disease?
Afterload reducing agents. These allow for more effective forward flow to occur despite a leaky valve -- they are not nearly as effective, or may not be effective at all, for a stenotic valve. Imagine a pump with a valve pushing water out of a hose in a pulsatile fashion. Imagine then that there was a leak in that valve. Now imagine someone went and crimped the hose -- what would happen? There would be more leakage backwards since the pressure would be higher in the hose. Afterload reducing agents decrease this backward pressure on the hose, and therefore more forward flow will occur with less work by the pump.
Diuretics. Diuretics may be prescribed if there is a tendency to "hold on to fluid" or if the patient has experienced congestive heart failure.
Digitalis. Digitalis increases the force of the heart muscle's contraction, and can be useful if the person has experienced congestive heart failure. Digitalis can also be useful for treatment of some arrhythmias, particularly atrial fibrillation, which can occur in valvular heart disease.
Blood pressure medications. Control of high blood pressure can be particularly important in people with valvular heart disease. This can decrease the amount of blood that leaks through regurgitant valves, and decrease the strain on chambers trying to pump through stenotic valves.
Blood thinners. Blood thinners, such as coumadin, aspirin, ticlodipine (Ticlid), clopidogil (Plavix), or dipyridamole (Persantine) may be prescribed. There may be a tendency to suffer from blood clots, resulting in strokes or other problems in some cases of valvular heart disease. This is more common in diseases of the mitral valve, particularly mitral stenosis. It is also an important consideration in persons who have atrial fibrillation, or who already have artificial valves.
Beta-blockers and anti-arrhythmics. Beta-blockers can be used for a variety of conditions. In the context of valvular heart disease, they are most often given for high blood pressure or irregular heart rhythms. Other types of antiarrhythmic drugs may also be prescribed.
What type of therapy is available?
What causes diseases of the heart valves?
Congenital heart disease. Problems with the heart valves may be present from birth. For example, the aortic valve may be almost entirely closed from a very early age. Much more common than this however, are mild abnormalities of the valve, such as being of made of two leaflets instead of three. This so-called "bicuspid aortic valve" is often associated with an accelerated incidence of aortic stenosis that may occur when the patient is in his or her fifties.
Rheumatic heart disease. Some infections with the bacteria called "streptococcus", particularly "strep throat" are followed in several weeks to months by a delayed inflammatory reaction called "rheumatic fever". The delicate valvular structures can be damaged at that time and progressive malformation of the valve can ensue over the next several decades. Valve replacement may be necessary in these later stages. Due to the discovery and use of antibiotics, rheumatic fever is far less common than in the past, particularly in developed countries. Proper treatment of strep infections can prevent almost all of the cases of rheumatic heart disease.
Specific damage from a heart attack. Specific parts of the heart muscle concerned with proper functioning of the valves can be injured in the course of a heart attack. If there is a tear of part or all of one of the "papillary muscles", severe mitral regurgitation can occur rapidly and require emergency therapy, perhaps including surgery.
Weakening of the supporting structures of the heart. In unusual cases, there may be a tear in one of the parts of the mitral valve which attach the valve to its papillary muscle. A rupture of some of the "chordae tendiniae" can cause substantial leakage through the mitral valve. This may begin and progress slowly, or be quite severe at the onset and require emergency surgery. Weakening of the walls of the aorta can occur, which leads to gradual dilation of the aorta, which can then lead to substantial leakage through the aortic valve.
Weakening of the heart muscle. When the heart muscle weakens, regardless of cause, it will tend to lengthen. As the chamber enlarges, so too do the holes which the Mitral and Tricuspid valves are designed to cover. At some point, while the valve itself is not diseased, it simply cannot cover this area, and valvular regurgitation will begin to occur. This often leads to yet further dilation and enlargement of the ventricles, and a "vicious cycle" begins to occur. When this is the cause of the leakage, surgery on the valve alone is often not helpful, since the primary problem was the diseased heart muscle in the first place.
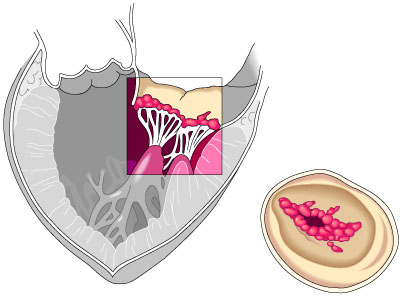
Infections. Infection of a heart valve is termed "endocarditis". This is not a common problem, but it can cause rapid progression of valvular disease, generally regurgitation, over a matter of days to weeks. This infection requires prompt diagnosis and treatment, but may still land up requiring valve surgery even when caught early.
Other causes. There are other even less common causes of valve disease (are you surprised?) which are not discussed here.
What is a heart "murmur"?
Murmurs can be caused by having a narrowed structure in the stream of blood, such as a stenotic valve. Likewise, the backward flow through a regurgitant valve occurs through a relatively small hole and causes sounds as well. The speed of flow is also increased in conditions such as exercise or fever, and this may cause straight or linear flow to become disrupted, even in normal structures. Thus, murmurs are common in this circumstance. Infants and children often have such sounds heard by medical professionals. When it is not caused by any abnormality of the heart, it is termed an "innocent murmur". The parent is generally told "not to worry about it" and that the "child will grow out of it". Both statements are correct when there is no underlying heart disease.
How can you tell if I have an abnormal valve?
The electrocardiogram is simply a representation of the electrical activity of the heart, and may show nothing at all about valvular problems, particularly in early or minor stages.
The chest x-ray, a relatively unsophisticated tool, can provide valuable information about the heart chambers and whether there is any evidence of congestive heart failure or other conditions.
An echocardiogram is a very valuable tool for evaluation of valvular heart disease. This is a non-invasive means of visualizing the heart muscle and valves using sound waves, or sonar. The valves can usually be visualized quite well, and the degree of leakage or stenosis can be estimated, in many cases with a high degree of accuracy.
Cardiac catheterization is sometimes needed to fully evaluate the heart valves, heart muscle, and heart arteries in some circumstances. Using this more "invasive" procedure, highly accurate information can be obtained.